by Eric Gahan
More and more as research develops and studies get published athletic trainers acquire tools to be more efficient and evidence based. One such tool established is the clinical prediction rule. Clinical prediction rules have been developed for many areas. One such area is the Canadian C-spine Rule (CCR) that has been published since 2003. With the publication of this clinical prediction rule we have evidenced based guidelines to send our patients for radiography of the cervical spine.
These guidelines give athletic trainers an evidenced based approach to sending an athlete for radiographs of the cervical spine.
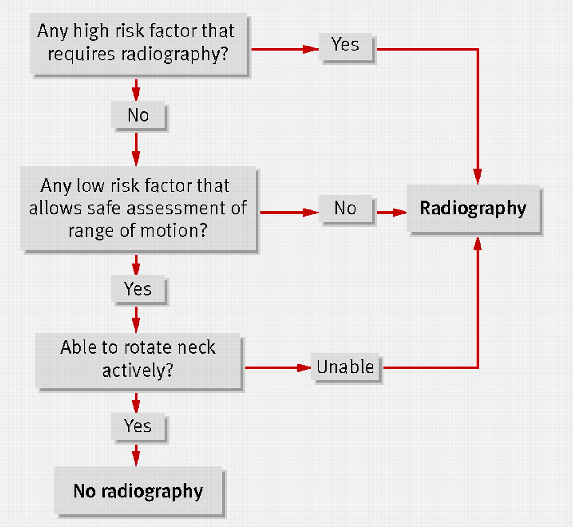
The CCR first evaluates suitable patients for any of three high risk criteria:
• The first of the three is an age-factor, deeming any patient who is 65 years old to be at high risk.
• The second factor looks for any dangerous mechanism, including a fall from a height greater than 3 feet, a high-speed motor vehicle collision (greater than 100km/hr, with or without rollover or ejection), an accident involving a bike or motorized recreational vehicle, or a direct axial load that would place the patient at high risk for a C-spine injury.
• The third high-risk factor is paresthesias in any or all extremities. If any of the three high-risk factors applies to the patient, the CCR mandates radiography.
If the patient lacks any high-risk factor, the CCR then evaluates the patient for the presence of any low-risk factor that will eventually allow for safe assessment of cervical range of motion.
• The published low-risk factors are simple rear-end motor vehicle collisions, a patient found sitting in the Emergency Department or ambulatory after the accident, delayed onset of neck pain or absence of any midline cervical pain. If none of these low-risk factors applies to the patient, the CCR mandates radiography.
If, however, the patient has no high-risk factor and does have at least one low-risk factor, the CCR then assesses the patient’s ability to actively rotate their neck, both left and right, at a 45° angle, with or without pain.
• If the patient is physically unable to perform this exercise, radiography is indicated. If the patient can perform this manipulation, however, the CCR recommends that no radiography is necessary to rule-out significant cervical spine injury.
There are several situations where the CCR could be utilized in your practice as an athletic trainer:
• Athlete is under cut while coming down from a dunk. Athlete lands on the head, cervical, and thoracic area of the neck and upper back. While clearing head and neck and calming the injured athlete the CCR flow cart could easily be used in your clinical on-court evaluation.
• Athlete is diving for a loose ball and collides with another player. This is a situation that could pass the athlete on the first area of the flow chart, but when assessing for cervical mid-line pain and also active rotation is not possible, you send for radiographs.
Given this clinical prediction rule we have peer reviewed research to make decisions requiring radiographs of the cervical spine. This is an area where error cannot come into our clinical practice and can only make us better. Of course with every clinical prediction rule it is important to remember these are only tools to help give efficient and effective health care to our athletic population. As the profession of athletic training continues to gain respect in the health care community it is important remember some words of wisdom shared with me as an athletic training student at Canisius College, “Always practice as a clinician and not a technician.”
Reference:
1. Bandiera G, Stiell, IG, Wells GA et al. The Canadian C-Spine Rule performs
better than unstructured physician judgment. Annals of Emergency
Medicine 2003; 42, 395-402.
2. Hoffman JR, Wolfson AB, Todd K, Mower WR. Selective cervical spine
radiography in blunt trauma: methodology of the National Emergency XRadiography
Utilization Study (NEXUS). Annals of Emergency Medicine
1998; 32, 461-9.
3. Stiell IG, Wells GA,Vandeheem K, et al. The Canadian C-Spine rule study
for alert and stable trauma patients. JAMA 2001; 286: 1841-8.
4. Stiell IG, Clement CM, McKnight RD, et al. The Canadian C-Spine rule
versus the NEXUS low risk criteria in patients with trauma. New England
Journal of Medicine 2003; 349: 2510-8.
5. Hoffman JR, Schriger DL, Mower WR, et al. Low-risk criteria for cervical-
spine radiography in blunt trauma: a prospective study. Annals of
Emergency Medicine 1992; 21:1454-1460.
6. Dickinson G, Stiell IG, Schull M, et al. Retrospective application of the
NEXUS low-risk criteria for cervical-spine radiography in Canadian emergency
departments. Annals of Emergency Medicine 2004;43: 507-514.
7. Viccellio P, Simon H, Pressman BD, et al. A prospective multicenter study
of cervical spine injury in children. Pediatrics 2001;108: e20.
8. State of Maine Spinal Assessment Protocol. Maine EMS 2002.
9. Hoffman JR, Mower WR, Wolfson AB, et al. Validity of a set of clinical
criteria to rule out injury to the cervical spine in patients with blunt trauma.
New England Journal of Medicine 2000; 343: 94-99.
10. Heffernan, DS, Schermer, CR, Lu, SW. What defines a distracting injury
in cervical spine assessment. Journal of Trauma Injury, Infection, and
Critical Care 2005; 59: 1396-1399.
11. Ngo, B, Hoffman, JR, Mower, WR. Cervical spine injury in the very elderly.
American Society of Emergency Radiology 2000; 7:287-291.
12. Eyre, A. Overview and Comparison of NEXUS and Canadian Spine Rules. American Journal of Clinical Medicine 2006; 3: 12-15.