By Art Horne


In a follow up from a previous post (Up The Chain It Goes), additional evidence supporting the relationship within the kinetic chain has emerged from south of the equator. In a study out of South Africa examining the link between available dorsiflexion and mechanical low back pain researchers found a statistically significant decrease in ankle dorsiflexion ROM and associated reporting of low back pain (Brantingham, 2006). With the vast majority of adults suffering from low back pain at some time in their life, (some reports are up to 85%) and 80% of people reporting foot problems during their lifespan, it’s not a surprise to see that these two conditions may very well be related.
Let’s take a closer look:
Methods: “ The study was a blinded, 2-arm, non-randomized clinical study involving 100 subjects with chronic or recurrent mechanical low back pain (intervention group) and 104 subjects without chronic mechanical low back pain (control group) between the ages of 18 and 45. A blind assessor performed weight-bearing goniometry of the ankle and big toe and the navicular drop test on all subjects in both groups.”
Results: “An independent t-test (inter-group) revealed a statistically significant decrease in ankle dorsiflexion range of motion in individuals with chronic mechanical low back pain.”
Conclusions: “This study’s data found that a statistically significant decrease in ankle dorsiflexion ROM, but not flatter feet, was associated with subject report of chronic mechanical low back pain disorders.”
Discussion: “The findings of this blinded study support previous reports suggesting that decreased ankle dorsiflexion may be a factor in chronic mechanical low-back pain. There was no clear association found between decreased hallux ROM and mechanical low back pain in this study. If these findings are confirmed through additional studies, exercise and manipulation therapy to increase ankle range of motion could become an important consideration in the treatment of some patients with mechanical low back pain disorders.”
Hmmm, if only we had some additional studies….
Perhaps this will help.
During a routine exit physical, 60 division one athletes were assessed for available weight bearing dorsiflexion bilaterally as described by Bennell et al in 1998 (inclinometer was replace by Clinometer app for ITouch) to examine limitations in this movement. Ten athletes with limited weight bearing dorsiflexion (less than 4 inches from knee to wall) volunteered for follow up evaluation and manual treatment. Out of the initial 120 measured ankles, 47 ankles (21 right, 26 left) demonstrated limited weight bearing dorsiflexion range of motion.
Athletes were then asked to walk normally in their athletic shoes while wearing an in-shoe pressure sensor (Tekscan) and through an optical measurement system (Optojump). Each athlete then underwent a general manual therapy intervention aimed to improve ankle dorsiflexion, followed again by the same gait analysis and pressure mapping data capture.

Gait Cliff Notes: optimal gait should have two mountains with a trough between them. The first mountain represents heel strike to midstance, the trough representing the mid-stance phase, and the second mountain being propulsion from full foot contact to toe-off.
Easy right? Good.
Note: The second mountain should almost always be higher than the first.
Case Study 1:
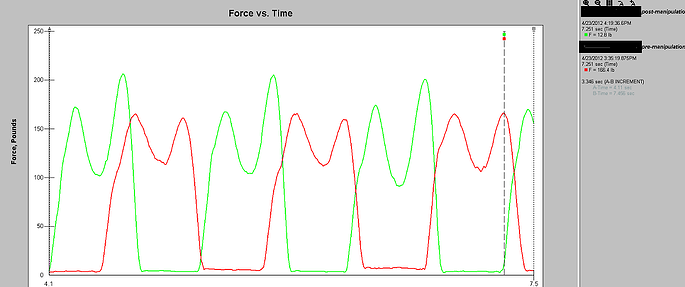
Pre-treatment (RED):
Notice how the first mountain is slightly higher than the second – this is BAD!
Remember from our cliff notes: the second mountain should be higher.
Post-treatment (GREEN):
Notice change in toe off from pre- to post-treatment which specifically targeted patient's limited dorsiflexion? The second mountain is now higher than the first. That’s a GOOD thing!
Awesome right?
Better yet – athlete was measured 3 days post treatment and improvement in Dorsiflexion range of motion stuck! Try doing that with a slant board stretch.
See Art Horne and Dr. Pete Viteritti discuss these and other changes at the foot and ankle, and how to assess and address soft tissue and bony restrictions in their presentation at the 2012 BSMPG Summer Seminar May 19-20th in Boston.

References
Bennell KL, Talbot RC, Wajswelner H, Techovanich W, Kelly DH and Hall AJ. Intra-rater and inter-rater reliability of a weight-bearing lunge measure of ankle dorsiflexion. Australian Journal of Physiotherapy. 44;175-180.
Brantingham JW, Gilbert JL, Shaik J, Globe G. Sagittal plane blockage of the foot, ankle and hallux and foot alignment-prevalence and association with low back pain. J of Chiropractic Medicine. 2006; 4(5); 123-127.

