By Art Horne
Your college anatomy teacher will have you believe that the knee is a simple hinge joint that’s only action is flexion and extension. Of course they probably mentioned the “screw home” mechanism and its related rotational component at some point, but this motion was most likely reviewed only as a side note to the main lecture with no further mention.
Unfortunately, this critical motion is often forgotten about during both the evaluation and rehabilitation of knee pain and for those with limited rotation in either direction, or an inappropriate axes of rotation, traditional knee pain management strategies aimed at limitations in flexion and extension will only lead to frustration.
Why care about tibio-femoral rotation?
Seriously?
Ignoring knee rotation and only examining the flexion-extension component is akin to checking the wheels on a train and then ignoring the tracks beneath them. Both are required if you’re hoping to efficiently move from A to B. So what happens when this critical motion is off? Inappropriate arthrokinematic motion will cause excessive motion or friction on adjacent structures – think train grinding around a corner and the screeching of wheels on the tracks.
“Fixed rotation of either the femur or tibia has a significant influence on the patellofemoral joint contact areas and pressures. This is due to the anatomic asymmetry in the knee with respect to all planes, as well as the laterally directed force vector that naturally exists in bipedal lower-limb biomechanics. Specifically, femoral rotation results in an increase in patellofemoral contact pressures on the contralateral facets of the patella, and tibial rotation results in an increase in patellofemoral contact pressures on the ipsilateral facets of the patella. This difference can be elucidated when one considers that rotation of the femur is biomechanically different than rotation of the tibia. For both tibial and femoral rotations, the patella’s distal attachment to the tibial tubercle influence the direction of patellar movement.” (Lee et al, 2003 p.686)
This influence on the patella by the relative motion between the tibia and femur is echoed by Kapandji,
“During movements of axial rotation the patella displacements relative to the tibia occur in a coronal plane. In the neutral position of rotation the patellar ligament runs a slightly oblique course inferiorly and laterally. During medial rotation the femur is laterally rotated with respect to the tibia, dragging the patella laterally, and the patellar ligament now runs obliquely inferiorly and medially. During lateral rotation, the opposite movements take place: the femur drags the patella medially and the patellar ligament now runs inferiorly and laterally with a greater obliquity than in the neutral position.”(Kapandji, pg.106)
“Patella displacements relative to the tibia are therefore indispensable for movement of both flexion-extension and axial rotation.”(Kapandji, pg. 106)
What exactly is happening?
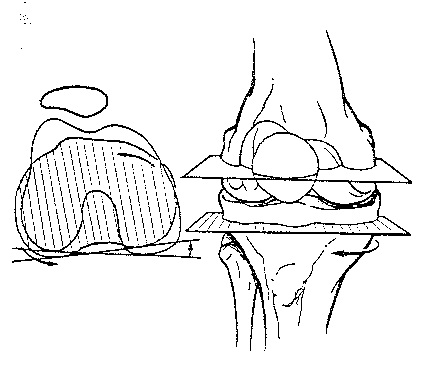
“During lateral rotation of the tibia on the femur the lateral condyle moves forward on the lateral tibial surface, while the medial condyle moves backwards on the medial tibial surface. During medial rotation of the tibia on the femur the converse is true: the lateral condyle moves backwards and the medial condyle forwards on their corresponding tibial surfaces. In reality, the anteroposterior movements of the condyles on their corresponding tibial surfaces are not identical.” (Kapandji, pg. 90)
Because of this unequal movement, the axis of rotation is NOT between the two intercondylar tubercles as many people would think, or what your college professor lead you to believe, but actually through the articular surface of the medial tubercle which serves as the central pivot point of the knee joint.
So now you’ve identified a limitation, how would you treat it?
Treatment Example: Below is an example taken from Greenman (Greenman’s Principles of Manual Medicine, Fourth Edition. Page 453), in an effort to restore normal tibia internal rotation
Position: Tibia Externally rotated
Motion Restriction: Internal rotation of tibia
- Patient is prone on the table with the operator standing at the side of the dysfunctional extremity
- Operator flexes the knee to 90 degrees and grasps the heel and the forefoot of patient.
- Operator dorsiflexes the ankle and internally rotates the tibia to the barrier.
- Patient externally rotates the forefoot against operator resistance for 3-5 seconds and three to five repeitions.
- Following each patient effort, the operator internally rotates the foot to the new barrier.
- Retest.
Are you treating Tibial rotation limitations in multiple stages of flexion?
Considering the obvious fact that the knee experiences a large excursion in flexion angles during sporting activity and also that patella contact pressures change as a result of knee flexion angle, (“Earlier in vitro studies have demonstrated that, in weight bearing, contact pressures within the patellofemoral joint increase as the knee flexes from 0 to 90 and decrease as the knee extends.” Lee, 2003), it is clearly warranted to treat limitations in both normal tibio-femoral along with patella and patellar tendon mobility in these various degrees of motion, and not simply in the traditional supine, table supported manner.
Closing Thoughts: Evaluating knee rotation is a critical part of any comprehensive knee pain evaluation, especially for those evaluations involving pain and swelling of a “non-specific” origin (aka: patellofemoral pain syndrome). For those that are familiar with the SFMA, limitations in multi-segmental rotation can be evaluated in a minimal amount of time and will lead you directly to this rotational component should a limitation exist. Treating this limitation should reflect the knee angle in which the restriction actually corresponds to.
Learn more advanced evaluation and rehabilitation techniques from the leaders in sports medicine and performance at the 2013 BSMPG Summer Seminar.
Register today before this event sells out!

References:
- Greenman’s Principles of Manual Medicine, Fourth Edition.
- Kapandji, AI. The Physiology of the Joints. Volume Two. The Lower Limb. Churchill Livingstone Elsevier. 2006.
- Lee TQ, Morriss G, Cstinalan R. The Influence of Tibial and Femoral Rotation on Patellofemoral Contact Area and Pressure. J Orthop Sports Phys Ther. 2003;33(11):686-693.
- Lee TQ, Yang BY, Sandusky MD, McMahon PJ. The effects of tibial rotation on the patellofemoral joint: assessment of the changes in in situstrain in the peripatellar retinaculum and the patellofemoral contact pressures and areas. J Rehabil Res Dev. 2001;38:463-469.
- Li G, DeFrate LE, Zayontz S, Park SE, Gill TJ. The effect of tibiofemoral joint kinematics on patellofemoral contact pressures under simulated muscle loads. J Orthop Res. 2004;22:801-806.

