The fusion of sports and medicine becomes a more potent mixture each day. Using tools that gauge performance with a high degree of accuracy allows us to quantify our results in almost any fashion imaginable. Tracking minute changes in the body such as heart rate, function, mobility and mechanics provides us information on our athletes that we can rely on to develop customized programs for each athlete. Real-time reporting functions provided by today’s latest technology make it simple and efficient to make evidenced based decisions in any setting.
Doctors, physicians and trainers are all working closely with one another to bring the most comprehensive care an athlete can hope for. Student athletes are among the top demographic to benefit from this union of sports and medicine where coaches and trainers regularly evaluate hundreds of students regularly. Coordinated care breeches team practices in addition to advising on lifestyle choices and curriculum.
Outside of institutions, merging is evident in private facilities where athletic development is the number one priority. Through the eyes of Dr. Thomas Lam, Director of Athletic Development at FITS Toronto, an environment focused on sports-science and coordinated care is a premier destination for training and therapy. Located in the hub of Canada, Dr. Lam’s two Toronto locations service every level of athlete, each equipped with a sports science lab. Tracking manipulations to the nervous system by evaluating the results in through changes to the biomechanical system, Evan Chait of Kinetic PT brings his discussion to OptoSource’s Fusion Track workshop.
For attendees of the Boston Sports Medicine & Performance Group, the Fusion Track will be the ideal chance to learn about incorporating data collection into sports performance planning and get a look at the best tools for managing all of the streams of information sports performance programs rely on today.
Speakers for this presentation include:
Dr. Thomas Lam of FITS Toronto on integrating objective analysis into an existing sports performance and medicine program.
Evan Chait of Kinetic PT will discuss The Chait Neuropathic Release Technique (CNRT), a multidisciplinary diagnostic and treatment process that focuses on 3 tiers of health. The 3 Tiers include the nervous system, biomechanical system, and the movement pattern system.
What to expect:
Using the cloud to safely and efficiently manage data.
Incorporating multiple streams of objective analysis into existing programs.
Tracking and trending change for coordinating care.
See this track along with 22 other lectures to choose from during our 2 day event this May 19th and 20th. A few seats remain - sign up before the last one goes!!!
Basketball is a multifactorial sport where recovery, nutrition, training, technical & tactical aspects, mental preparation and innate conditions are involved. As S&C coaches, our ultimate goal is to enhance the team performance by optimising each player´s physical condition and helping them stay away from injuries.
Profiling athletes is an important part of the training process that helps me to decide what is the most appropriate strategy for each of the players I coach.
The image below represents the average results of 3 pre-season assessments to determine the % of Type I muscle fiber (Slow Twitch). It is an example of two different football players, both of them playing for the same team but with a different muscular profile.
The player on the left seems to have lower predominance of slow twitch as every muscle group except Semitendinosus (very postural muscle) is within 30-45% of slow muscle fibres.
The player on the right seems to have higher predominance of slow twitch, especially on key muscle groups like Biceps Fem (59,8%) and Gluteus Max (62%).
Take a sneak peek into Bruce Williams' presentation, New Concepts in Foot Function & Gait Analysis Assessments & Treatments, at the 2012 BSMPG Summer Seminar.
Space is still available - Register today before the last seats are gone!
Most athletes and coaches think podiatrist means someone who makes orthotics, could you dispel that myth and talk about the holistic approach with foot care and how you even work with injuries in the low back? Many don't understand your profession deals with biomechanics, surgery, and even manual therapy.
Podiatry is a very interesting profession. Surgery is really the highlight of what Podiatrists do and are trained to do at the present time. All Podiatrists receive about a year of biomechanics while in school. They are all trained to cast for orthotics and write prescriptions as well. Some podiatrists utilize manual therapy in their practice, but probably less than 5%.
In my practice I figured out very quickly my orthotic outcomes were not what I wanted them to be. I set out to understand how I could do a better job for my patients and that lead me down a very interesting path of self- education. I found a mentor to assist me in the use of in-shoe pressure and video capture technology. He also happened to expose me to the use of manual therapy in the foot and ankle. The use of the technology and the therapy really opened my eyes to what I was missing in practice. The use of the quantitative data from the in-shoe pressure really exposed me to the way the foot will function and react to a shoe and to an OTC or custom foot orthosis. This has helped me to realize my limitations in practice while also allowing me to move past most of my peers in the understanding of the foot’s importance in walking, and athletic gait.
Most of my sports medicine podiatry peers are great collaborators with physical therapists, strength and conditioning coaches, athletic trainers and massage therapists. We all realize that we are just a piece of the puzzle in the process of enabling our athletes to compete at their highest levels.
Barefoot training and minimalist shoes seem all the rage right now, can you share some objective pros and cons to what athletes may benefit and risk wise when diving into this territory?
Barefoot is the thing right now, just as toning / rocker bottom shoes were a few years back. In moderation and in certain specific situations I see benefit for patients and athletes from both types of shoes. The biggest problem I have with the minimalist / barefoot shoe debate is that there is very little proof that doing workouts barefoot will have the amazing results that so many people say they have had.
I use a lot of technology to quantitate my outcomes, good or bad. I would appreciate it if others would utilize similar technology to do the same. Enthusiasm is wonderful, but there is a need to realize when something is not working the way we hoped it would and realize a different take is needed to get a successful outcome. I have seen a lot of people chasing rainbows the last few years and it confuses me. I appreciate the capacity of strength and conditioning to improve outcomes for athletes, but, there are limitations to what can be achieved and maintained. I see the limitations daily with what I do and I try to refer to P.T. and strength coaches to assist my patients and athletes to achieve an overall better outcome.
I am regularly amazed that so many in the sports industry seem very anti-foot. I’m not really sure why this is, but my suspicion is that every podiatrist and many P.T.’s will put patients and athletes in an orthotic and often they do not work. Podiatrists are very bad about this and often don’t have a specific reasoning or a plan for why they chose to use their devices. I have a very specific reasoning pattern and evaluation process for doing what I do for my patients. I really try to have a method to my madness. I have a very good success rate, but not perfect by any means. I am always looking for a new way to improve my outcomes whether it is through a new modification to a device, a new mobilization technique or through partnering with a better team of sports minded individuals so that we can all work together to benefit our athletes.
When the foot hits the ground a complex reaction of joints, muscles, and neurological responses happen. Could you share your approach with both technology and experience when working with athletes?
I use F-Scan in-shoe pressure and Dartfish as well as another older video capture technology. I am starting to experiment with wireless emg and a nodular motion capture technology. In-shoe pressure can give you a tremendous amount of insight into how an athlete’s foot and lower extremity functions. There are however limitations to what the data can indicate. This is why I use video capture and why I’m experimenting with the nodular motion capture. It is important to know what the position of the hips, knees and lower extremity in general are doing for each step. Relating this to the trunk position can give you insight as well. Once you have enough gait data from the trunk on down, then you can really start to incorporate a plan for the athlete from the ground up. As you track going forward you should see what is working and what is not.
Wearable technology is being used now and will be utilized even more in the near future. It is important to start to work with this technology or to partner with those who do use it regularly. There are great benefits to quantifying evaluations and using wearable tech to validate plans of interventions is going to become the gold standard as we move forward.
You are familiar with different screens such as the FMS and traditional orthopedic assessments. Could you share your perspective on how some additional information from your methodology can help athletes reduce injuries?
FMS is a great screening tool and can give you quite a bit of information to help practitioners to formulate a plan for an athlete’s rehab or for their regular conditioning.
I have a basic screening tool that can assist or expand on the FMS as far as for evaluating the foot, ankle and lower extremity. If you can gain a better understanding of how the foot is structured and functions then you can start to get a much better understanding of how your interventional plans will work and whether you can expect realistic improvement.
I like to use a basic scale to discern the structure and stiffness of the foot along the medial and lateral columns. It is good to know the standing heel position of the foot, if there is any limb length difference left to right, and also the available range of motion of the big toe joints and the ankle joint. Just having these few basic points of information can start to give insight to why an athlete may be prone to stress fractures of the metatarsals, chronic ankle sprains, and even if they may be prone to knee injuries. Adding ranges of motion of the hips, and knees in static and walking gait can multiply your available knowledge base even more.
There are reasons and patterns for why some athletes get injured and why some do not. Quantifying as much of the structural components of the foot and lower extremity function is the best way to start to identify those patterns.
But for all the things and subject matter they disagree about, there is one thing that every coach certainly would agree on.
It's not sets or reps.
It's not the use of Olympic lifts, or periodization method, or even conditioning protocols.
No.
The one thing that all coaches agree on is the struggle to program and plan for large number numbers of athletes in a consistent and easy manner.
It's the one thing that ALL strength coaches would agree upon.
And now, thanks to Cal Dietz and XL Athlete, coaches can spend more time on the floor coaching and less time plugging numbers into excel files or adjusting programs because of an athlete's injury or because a sport coach changed training times.
Click HERE to learn more about the XL Strength Program Developer.
See Cal Dietz along with more of the nation's top hockey strength coaches and keynote speakers including Craig Liebenson and Chris Powers at the 2012 BSMPG Summer Seminar this May 19th and 20th.
See Highlights from Coach Dietz's talk at the 2011 BSMPG summer seminar below.
There are only two weeks remaining before our 2012 BSMPG Summer Seminar, May 19th and 20th!!! We are almost at capacity, so register today before the last remaining seats are scooped up!
DO YOU WANT TO BE A LUCKY WINNER??
BSMPG will be hosting a VIP gathering Friday, May 18th during the afternoon and early evening featuring:
Seminar speakers, performance coaches from the NBA & NHL, college strength coaches from the top programs across the country, select area athletic trainers, and physical therapists as well as representatives from the top sport science companies... and hopefully YOU!!!
This is a closed event but BSMPG is opening its doors to 8 lucky registrants.Register prior to Friday, May 11th at Midnight and be eligible for additional lectures and breakout sessions Friday afternoon. In addition, winners will be invited to our pre-seminar speaker social Friday night!
What happens if I don’t get my name picked?
Don’t worry – with BSMPG everyone is a winner! Join seminar speakers and attendees for a post-seminar social Saturday night at Symphony 8 Bar and Restaurant immediately following the last lecture of the day. Hey... learning is hard work and you deserve some food and drink provided by OPTOSource.
Attendees will also be placed in a drawing for a chance to win sponsor prizes! Where else can you get free gear and free food?
Pre-Season Screening for Sport May 18th 4:00 - 5:15 pm
During the afternoon Jose Fernandez and Dr. Bruce Williams will do a live assessment of an athlete, followed by group discussion on best practices with screening. A focus on gait and lower body mechanics is the highlight, supported by both biochemical and biomechanics monitoring. Evidence based medicine and the latest advancements of technology, therapy, and sports performance methods will be covered. With the advent of Moneyball, Jose and Bruce will show how they look at risk analysis with athletes in team sports from both a time management perspective and decision making process.
Speaker Social to follow.
Winners will be informed of locations and additional details after drawing.
Friday Social Sponsored by:
TopCoder is the world’s largest competitive Open Innovation Community of digital creators with over 400,000 members representing algorithmists, software developers and creative artists from over 200 countries. The TopCoder Community creates digital assets including analytics, software and creative designs and solutions for a wide-ranging client base through a competitive, rigorous, standards based methodology. Combined with our extremely talented Community this groundbreaking methodology results in superior outcomes for our clients. For more information about sponsoring TopCoder events and utilizing TopCoder’s software services and platforms, visit www.topcoder.com.
In a follow up from a previous post (Up The Chain It Goes), additional evidence supporting the relationship within the kinetic chain has emerged from south of the equator. In a study out of South Africa examining the link between available dorsiflexion and mechanical low back pain researchers found a statistically significant decrease in ankle dorsiflexion ROM and associated reporting of low back pain (Brantingham, 2006). With the vast majority of adults suffering from low back pain at some time in their life, (some reports are up to 85%) and 80% of people reporting foot problems during their lifespan, it’s not a surprise to see that these two conditions may very well be related.
Let’s take a closer look:
Methods: “ The study was a blinded, 2-arm, non-randomized clinical study involving 100 subjects with chronic or recurrent mechanical low back pain (intervention group) and 104 subjects without chronic mechanical low back pain (control group) between the ages of 18 and 45. A blind assessor performed weight-bearing goniometry of the ankle and big toe and the navicular drop test on all subjects in both groups.”
Results: “An independent t-test (inter-group) revealed a statistically significant decrease in ankle dorsiflexion range of motion in individuals with chronic mechanical low back pain.”
Conclusions: “This study’s data found that a statistically significant decrease in ankle dorsiflexion ROM, but not flatter feet, was associated with subject report of chronic mechanical low back pain disorders.”
Discussion: “The findings of this blinded study support previous reports suggesting that decreased ankle dorsiflexion may be a factor in chronic mechanical low-back pain. There was no clear association found between decreased hallux ROM and mechanical low back pain in this study. If these findings are confirmed through additional studies, exercise and manipulation therapy to increase ankle range of motion could become an important consideration in the treatment of some patients with mechanical low back pain disorders.”
Hmmm, if only we had some additional studies….
Perhaps this will help.
During a routine exit physical, 60 division one athletes were assessed for available weight bearing dorsiflexion bilaterally as described by Bennell et al in 1998 (inclinometer was replace by Clinometer app for ITouch) to examine limitations in this movement. Ten athletes with limited weight bearing dorsiflexion (less than 4 inches from knee to wall) volunteered for follow up evaluation and manual treatment. Out of the initial 120 measured ankles, 47 ankles (21 right, 26 left) demonstrated limited weight bearing dorsiflexion range of motion.
Athletes were then asked to walk normally in their athletic shoes while wearing an in-shoe pressure sensor (Tekscan) and through an optical measurement system (Optojump). Each athlete then underwent a general manual therapy intervention aimed to improve ankle dorsiflexion, followed again by the same gait analysis and pressure mapping data capture.
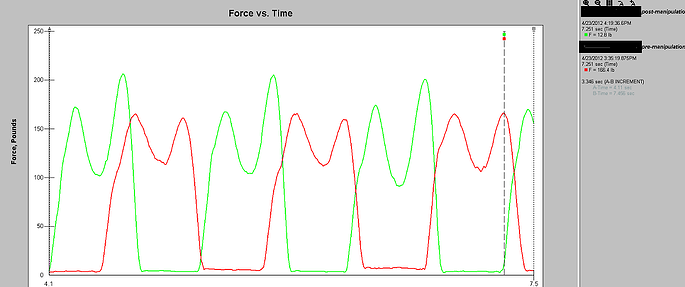
Gait Cliff Notes: optimal gait should have two mountains with a trough between them. The first mountain represents heel strike to midstance, the trough representing the mid-stance phase, and the second mountain being propulsion from full foot contact to toe-off.
Easy right? Good.
Note: The second mountain should almost always be higher than the first.
Case Study 1:
Pre-treatment (RED):
Notice how the first mountain is slightly higher than the second – this is BAD!
Remember from our cliff notes: the second mountain should be higher.
Post-treatment (GREEN):
Notice change in toe off from pre- to post-treatment which specifically targeted patient's limited dorsiflexion? The second mountain is now higher than the first. That’s a GOOD thing!
Awesome right?
Better yet – athlete was measured 3 days post treatment and improvement in Dorsiflexion range of motion stuck! Try doing that with a slant board stretch.
See Art Horne and Dr. Pete Viteritti discuss these and other changes at the foot and ankle, and how to assess and address soft tissue and bony restrictions in their presentation at the 2012 BSMPG Summer Seminar May 19-20th in Boston.
References
Bennell KL, Talbot RC, Wajswelner H, Techovanich W, Kelly DH and Hall AJ. Intra-rater and inter-rater reliability of a weight-bearing lunge measure of ankle dorsiflexion. Australian Journal of Physiotherapy. 44;175-180.
Brantingham JW, Gilbert JL, Shaik J, Globe G. Sagittal plane blockage of the foot, ankle and hallux and foot alignment-prevalence and association with low back pain. J of Chiropractic Medicine. 2006; 4(5); 123-127.
In the classic model for the care of student athletes, sports medicine and performance training services are provided under the supervision of the athletics department. This has been challenged recently with suggestions of alternate organizational schemes, including at Boston University, where oversight of athletic training services was transferred from athletics to college health, arranging athletic training services into “medically-oriented units.”
At Boston University, they noted some key advantages: delivery of superior health care services, improved on-going educational opportunities for staff and students, and enhanced working conditions for athletic trainers.
In 2011, here at Northeastern University we followed suit, placing both athletic training and performance services under the direct supervision of sports medicine personnel. The head team physician for the university provides oversight for a dual-trained athletic trainer and strength coach who directs these sports performance services. These changes were in response to difficulties we had observed, including an apparent lack of standardization of services, especially related to prevention models provided by athletic training and strength and conditioning.
Also apparent were communication breaches between and among the coaching staff, strength and conditioning personnel, sports medicine providers, and the student-athletes who were receiving care from these individuals.
So university authorities agreed to implement a new model for the care of student athletes that placed athletic training as well as strength and conditioning under the supervision of sports medicine. This allowed us to consider the potential advantages as well as challenges that will be encountered as the model is implemented.
One clear advantage is to improve collaboration during pre-participation screening for athletes. In 2007, the NCAA mandated that all student athletes receive a pre-participation examination (PPE) by medical staff prior to engaging in collegiate sports.
There is a reason why top athletes and clubs from around the world seek out Bill Knowles after surgery. He is simply one of the best in the world at returning athletes to pre-surgery performance levels.
Meet Bill Knowles at the 2012 BSMPG Summer Seminar, May 19-20th as he lectures about Reconditioning and Return to Competition Strategies for the Joint Compromised Athlete.
England FA, Manchester United, Chelsea, Manchester City, Tottenham, Aston Villa, Bolton Wanderers, Middleborough, West Brom
England Rugby(RFU), Scotland Rugby(SRU), London Wasps, Leicester Tigers, London Irish, Harlequins, Sale Sharks, Edinburgh
US Ski Team, Canadian Ski Team, Edmonton Oilers, Indianapolis Colts, San Jose Sharks
Athletic Development Coach and Sports Rehabilitation Specialist Certified Athletic Trainer, Certified Strength and Conditioning Specialist
Experience: • 21 years professional experience working with World-class, Olympic, Professional, Elite, & Nationally ranked athletes from around the world. • Professional and World-Class sports include: Soccer (football), Rugby Union, Ice Hockey, Basketball, Football, Aussie Rules Football, Golf, Alpine and Freestyle Mogul Skiing, Snowboarding and Swimming •Former Head Athletic Trainer and Director of Strength and Conditioning at Burke Mountain Academy (Vermont, USA) for 12 years. BMA is recognized historically as the best youth sports academy in the world for alpine ski racing. The list of Olympic, World Cup, and World Junior success is unparallel in the Unites States and worldwide. • Author of numerous articles on injury prevention and performance training in ski publications, strength and conditioning magazines and health journals. • Featured speaker dozens of times around the United States, Canada, England and Scotland on topics related to injury reduction programs, rehabilitation/reconditioning, and performance training for all types of athletes.
For the past 21 years Bill Knowles has been working with elite level athletes from around the world. As a sports rehabilitation specialist, Bill has helped Professional and Olympic level athletes recover from season ending and career threatening injuries. His energy and enthusiasm keeps every training session educational and fresh, while his unique experiences allows a creative approach to address any injury situation. Bill’s rehab philosophy allows each athlete the opportunity to express their inherent athletic ability quickly following injury or surgery. This mean the “down time” is minimal and the athlete stays very active and motivated.
After receiving his education at Cortland State College in New York, Bill began his career at the world renowned sports academy for Alpine and Nordic ski racing; Burke Mountain Academy. As the Head Athletic Trainer and Performance Director Bill took care of countless knee injuries and developed his skills that began to attract world-class ski racers from Europe and North America. Since then athletes from England, Scotland, Ireland, and Australia have visited Bill in Killington, Vermont. Bill has also traveled extensively working with and visiting many of the top sports clubs in the world.
This success has evolved to designing and implementing rehab and performance programs that have placed athletes back into the English Premiership and Championship Football Leagues, The Rugby World Cup and Premiership Squads, Baseball World Series, Winter Olympic podiums and X-Game podiums.
As a former collegiate soccer player, ski racer, and coach, Bill delivers his training programs they way an athlete understands and respects.
“The residents who live here, according to the parable, began noticing increasing numbers of drowning people caught in the river’s swift current and so went to work inventing ever more elaborate technologies to resuscitate them. So preoccupied were these heroic villagers with rescue and treatment that they never thought to look UPSTREAM to see who was pushing the victims in.”
Learn what is hurting your feet and your performance, and how to finally train your feet the way they were meant to be.



















{kind=link}